Reproductive And Child Health (RCH) II Programme : Service NGO Scheme
“Reaching the unserved for Quality Reproductive Child health services”.The Reproductive and Child Health (RCH) II programme launched by Government of India (GoI) envisages providing quality services and achieving multiple objectives. It ushered a positive paradigm shift from method-oriented, target-based activity to providing client-centered, demand-driven quality services. The Reproductive and Child Health (RCH) Program being implemented by Ministry of Health & Family Welfare (MOHFW) through Service NGOs, supports various interventions aimed at enabling clients to receive clinical services, councelling and education for responsible health and sexual behavior, access user-friendly services for maternity care, child survival, to make informed choices, preventing unwanted Pregnancy and safe abortion and management of reproductive tract infections and sexually transmitted diseases.
Ministry of Health and Family Welfare-Government of India & NRHM Cell, Government of Maharashtra, State Family Welfare Bureau, Government of Maharashtra and Pune District Integrated Health Society had entrusted Lokmanya to implement SNGO Scheme in Khed (Block) Taluka of Pune District for the period of three years duration from 2010 to 2013. To improve health status of vulnerable population by ensuring accessibility and availability of quality primary health care and family welfare services to them.
The following are the key indicators that are covered under SNGO project.
- Mother & Child Health Care (MCH): to ensure full ANC coverage; to improve institutional deliveries and to provide PNC care and essential neo-natal care,
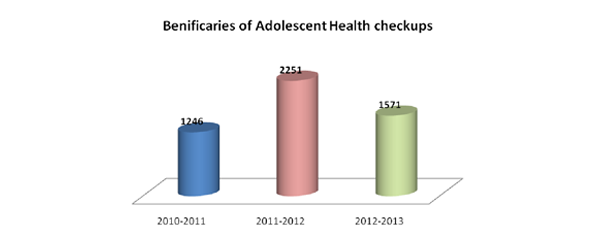
- Adolescent Health Care
- Prevention and treatment of Malnutrition
- Family Planning and Councelling services : meeting the unmet need for family planning
- RTI \STI Management.
- Hygiene and sanitation and capacity building of PRI representatives.
Lokmanya also focused on integrating Aaganwadi workers, VHC members, RKS members and Community Based Organization with RHC II programs.
The overall objective of the SNGO Scheme is to
- To improve the accessibility, availability and acceptability of RCH services by providing preventive and clinical services in an integrated and participatory manner.
-
Improving the aggregate indicators towards achieving the expected results set under SNGO Project by the end of 2013.
- To increase full ANC coverage from 28% to 80%
- To increase institutional delivery from 71% to 90%
- To reduce the malnutrition cases
- To provide Family Planning services
- To Provide RTI/STI management services
- To reduce the Percentage of anaemia cases among adolescent girls.
Project Strategic
- Regular Free Mobile services in the community
- ANC services through mobile clinics at community, hospital and PHC
- Specialized Gynecological /Pediatric services at the PHC
- Hospital based referral services at Lokmanya Hospital & other Private affiliated Hospitals
- Emergency services at hospital through specialist
- Adolescent health services
- Medical intervention and supplementary food for malnourished children Contraception services – Spacing and sterilization of the eligible couples
- Specialized Camps for RTI/STI & FP in the community
- Syndromic management of RTI/STI cases.
- Partnership networking and linkages with NGOs; CBOs
- Human Resource Development, Monitoring and Documentation
Indicator Wise Comparative Analysis Of Base Line & End Line Survey
As per the SNGO guidelines the progress of the Service NGO was measured against a cluster of indicators selected and included in their baseline survey and the project proposal. The Base line and End line cross sectional studies was conducted by drawing samples to represent the project intervention area in each PHC as well as community cluster. These surveys were designed to facilitate both project evaluation (at start-up and completion) and periodic monitoring during implementation. The design of the study consisted of a quantitative survey and a qualitative approach using in-depth interviews and focus group discussions.
The comparative Base line and End line survey was conducted to collected data on demographic characteristics of the household, Maternal and Child Health (MCH): Antenatal Care (ANC) and Institutional delivery, Child Immunization, Family Planning (FP), Reproductive Tract Infections (RTI)/ Sexually Transmitted Infections (STI), Adolescence Reproductive & Sexual Health (ARSH) to access the improvements in the service delivery and the results in a given area of intervention. The comparative analysis of base line & end line survey is presented here.
| Indicator | Description | Baseline Survey 2008 Percent | End Line Survey 2013 Percent |
|---|---|---|---|
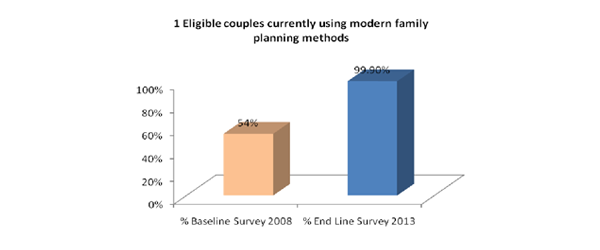
| 1 | Eligible couples currently using modern family planning methods | 54 | 99.90 |
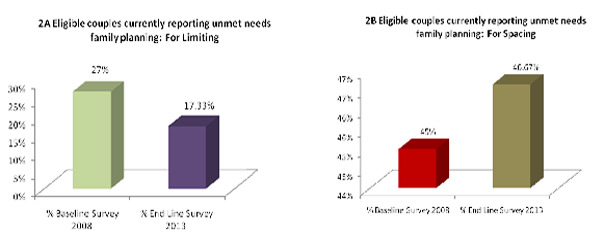
| 2A | Eligible couples currently reporting unmet needs family planning: For Limiting | 27 | 17.33 |
| 2B | Eligible couples currently reporting unmet needs family planning: For Spacing | 45 | 46.67 |
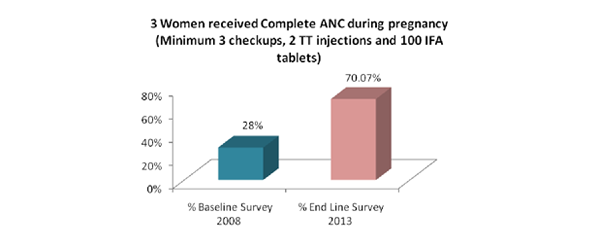
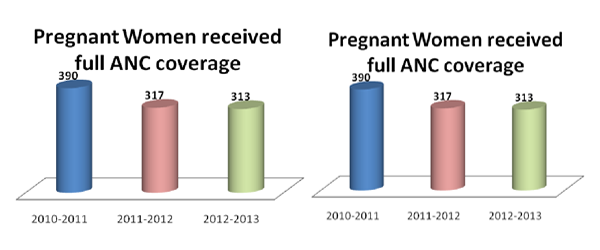
| 3 | Women received Complete ANC during pregnancy (Minimum 3 checkups, 2 TT injections and 100 IFA tablets) | 28 | 70.07 |
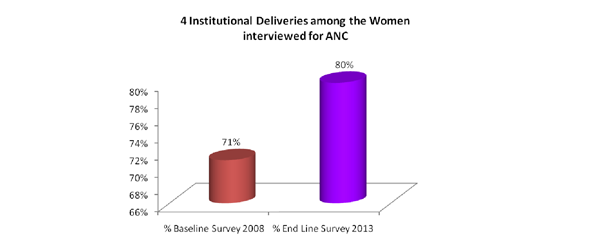
| 4 | Institutional Deliveries among the Women interviewed for ANC | 71 | 80.00 |
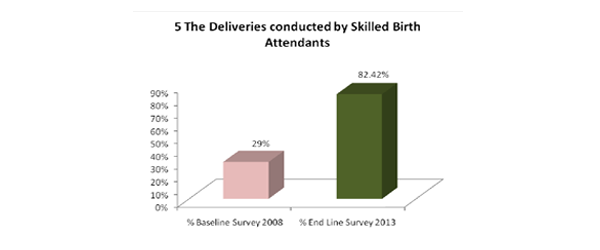
| 5 | The Deliveries conducted by Skilled Birth Attendants | 29 | 82.42 |
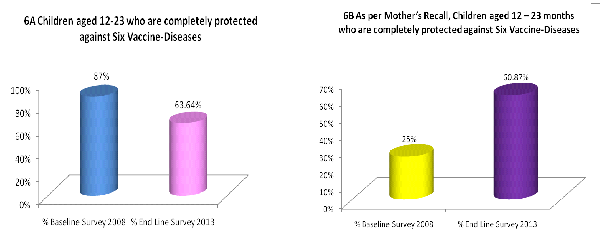
| 6A | Children aged 12-23 who are completely protected against Six Vaccine-Diseases | 87 | 63.64 |
| 6B | As per Mother’s Recall, Children aged 12 – 23 months who are completely protected against Six Vaccine-Diseases | 25 | 60.87 |
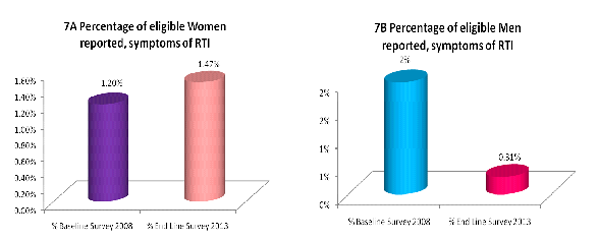
| 7A | Percentage of eligible Women reported, symptoms of RTI | 1.2 | 1.47 |
| 7B | Percentage of eligible Men reported, symptoms of RTI | 2 | 0.31 |
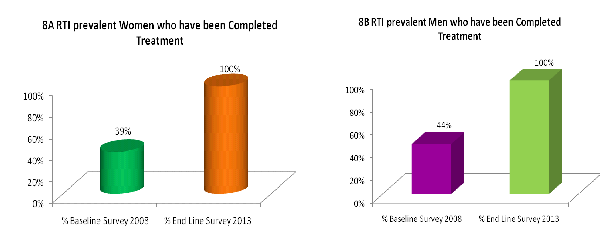
| 8A | RTI prevalent Women who have been Completed Treatment | 39 | 100.00 |
| 8B | RTI prevalent Men who have been Completed Treatment | 44 | 100.00 |
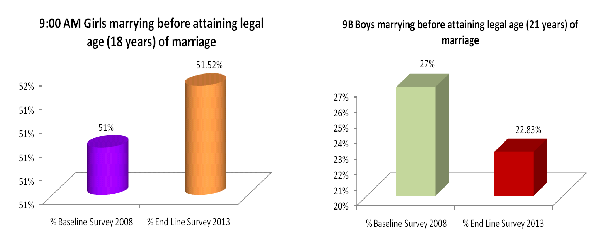
| 9A | Girls marrying before attaining legal age (18 years) of marriage | 51 | 51.2 |
| 9B | Boys marrying before attaining legal age (21 years) of marriage | 27 | 22.83 |
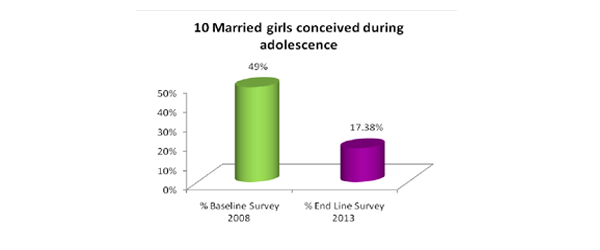
| 10 | Married girls conceived during adolescence | 49 | 17.38 |
Indicator #1: Eligible Couples Currently Using Mordern FP Method
Indicator 2: Unmet Need Spacing & Unmet Need limiting
Indicator 3: Women received complete ANC during Pregnancy
Indicator 4: Institutional Deliveries.
Indicator 5: Deliveries conducted by skilled attendants
Indicator 6: A & B as per immunization record & Mothers recall.
Indicator 7: RTI prevalence among women & Treatment sought for RTI symptoms
Indicator 8: Eligible women completed treatment & Both completed treatment
Indicator 9: 9 (women & Men started living together.)
Indicator 10: (women conceived during adolescent)
To conclude these data indicate that significant progress has been made in almost all the key indicators in the project intervention area. However sustained efforts are required to ensure 100% full ANC coverage, Full Immunization and institutional deliveries in the inaccessible remote villages.
Service NGO Scheme Project Activity Report
Period: June 2010 to May 2013Activities Carried Out
- Prior to implementation of the project, we conducted Project Area remapping and facility survey to understand the challenges and indentify the gaps. ( See Annexure)
- The project intervention strategy was discussed with Medical Officer PHC and THO of the project area and project implementation plan was chalk out.
- Area Specific and indicator specific activities were drawn for actual implementation.
Sensitization Workshop For Stakeholders
With an objective to create aware about the project goal and objective all the stakeholders were involved and a workshop on SNGO Scheme were organised in the Khed Block. This has help us to develop good rapport and will enabled us to bring about a situation where the people shall genuinely feel that they own the project and ultimately empower them to take charge of it in long run.

- 100 SHG group members were sensitized about the SNGO programme and services that will be provided under the scheme.
- Networking with SHG group is established for 100% registration of ANC / PNC cases. A Special Sticker drive was initiated in 30 villages. These groups were sensitized for Identification of ANC/PNC cases, eligible couple and information pamphlet with emergency number of Lokmanya & the details of services available at Lokmanya Hospital Chandoli was distributed.
Interaction With Panchayat Raj Institute Representative On RCH

Meeting with Sarpanch of project intervention villages were conducted by project staff and appraised about the SNGO Scheme and their roles were discussed.
- 56 villages were visited by SNGO Coordinator.
- The basic objective of this training is to strengthen the role of PRI members on the issues related to health, with specific reference to Service NGO Scheme and the role of PRI members in implementing the new strategy on RCH Services, functions of Village Health Committee, and Gender Issues.
Sensitization Of Community Health Workers: ASHA / PADA Workers
Success of SNGO Scheme is dependent upon committed and motivated health & community workers who work closely with the communities. One of the key strategies under the NRHM is having a community health worker that is ASHA (Accredited Social Health Activist) for every village with a population of 1000. The ASHA has to work in the community for the rural poor.
- ASHA and PADA workers training workshop was conducted for discussing the strategies for ensuring 100% registration of ANC / PNC cases. Their activities include registration of pregnancies, deliveries, newborn children, morbidity and mortality records. They also follow pregnant women, 0-3 year olds and any other specific groups as and when so identified.

Sensitization Of Anganwadi Workers
- One day workshop for Anganwadi workers was organized in the month of June at Lokmanya Hospital Chinchwad for apprising about the SNGO Scheme their role and strategies for controlling Malnutrition in the area was discussed. Public Health Specialist delivered the talk. This Workshop was attended by 52 anganwadi workers.
- Various tools adopted for training include group work, flip chart presentations, panel discussions and field visits
Household Micro Planning
With an Objective to enumerate all the project beneficiaries and Micro planning of the intervention strategies for the Identification of the Pregnant and Lactating mother, early Registration & for providing Follow -up Services to the project area covering every household. This was implemented by a specially designed yellow sticker which was pasted on the doors of the beneficiary. Accordingly Area Mapping was done and information on RCH demand generation was disseminated. To strengthen the household planning, 30 parivartaks (Voluntary peer educators) were trained and involved in this activity. Each parivartak is responsible for 10-15 families in their neighborhood; dissemination of information, pasting stickers, follow-up of Filling up of prescribed format with 3 consecutive month’s recall of menstrual cycle.
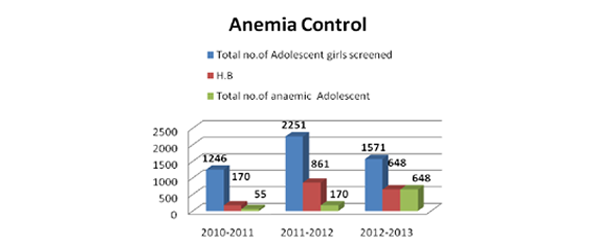
Adolescent Girls Anaemia Control Program
Lokmanya initiated the “Adolescent Girls’ Anemia Control Program” for the adolescent girls in all the secondary and higher secondary sections of SNGO Project Area from November 2010.
Program Aims

- To institute school/Jr. College based, supervised weekly IFA supplementation with an in-built compliance monitoring system.
- To provide nutrition education to the beneficiary girls and teachers in order to effectively modify dietary behavior and thereby improve the intake of iron available from the food.
Program Objectives
- To ensure that 90% of adolescent (12-19 year) girls in schools/ colleges and 70% of out-of-school participate in weekly consumption of IFA tablets under supervision
- Anemia prevalence in adolescent girls reduced by 90% by the end of the project period (three years).
- Improved dietary practices are observed in at least 25% of the adolescent girls both in and out of school setting by project end.
The program is operational in 12 schools & Colleges covering over 600 adolescent schoolgirls as beneficiaries in the first phase. Programme sensitizations in Schools in completed and about 70% of the schools have sent their consent to participate in this programme. The second phase of the program will be initiated in other remaining schools from July 2011, in which the strategy is reaching out-of-school girls through schoolgirls using girl-to-girl approach.

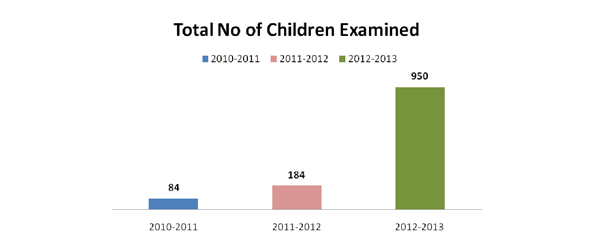
0-6 Children And School Health Check-Up Camps:
-
Child health Check-up camp was organized at 20 villages. 134 Children were examined and treated for upper respiratory infection and other illness.
-
School Health Check-up Camp organised at Middle & Higher Secondary School: Pait, Kadus.


Vande Mataram Campaign
The morbidity and mortality of maternal health in khed taluka Study indicates that the major causes of maternal mortality are ante and post partum hemorrhage, anemia, obstructed labour, hypertensive disorders, post partum sepsis and unsafe abortions and quick repeated pregnancies. Deaths due to anemia, obstructed labour, hypertensive disorders and sepsis are preventable with provision of adequate antenatal care, referral and timely treatment of complications of pregnancy. District Household Survey shows that about 33% pregnant women do not avail of even a single ante natal check up.
Antenatal care such as iron supplementation and infection screening, skilled care during birth in the community and at facilities as well as basic postpartum and newborn care during the first few weeks of life can benefit mothers and babies, and can save lives. Research indicates that if women had access to basic maternal health services, 80% of maternal deaths could be prevented.
To bridge this gap we have developed and launched Vande Mataram Campaign with the help of five private practitioners. This scheme envisages provision of free screening for risk factors including ante natal check up to all pregnant women, mapping the delivery place, IEC (information, education and communication) and family planning counseling of new mothers regularly by the public and private facilities on a fixed date of 9th of each month. This has improved the access of pregnant women to ante natal check up and thus, reduce maternal and neonatal deaths significantly.
Indicator Specific Activity: Mother And Child Health Service
Ensuring safe motherhoodSafe motherhood means ensuring that all women have access to the information and services they need to go safely through pregnancy and childbirth. This included:
- Education on safe motherhood
- Prenatal care (care during pregnancy) and counseling with focus on high risk pregnancies
- Promotion of maternal nutrition
- Adequate delivery assistance in all cases
- Provisions for obstetric emergencies including referral services for pregnancy, childbirth and abortion complications
- Postnatal care(care after the child birth)
Antenatal Care
woman in order to make the outcome of pregnancy safer, reduce cases of maternal morbidity and mortality through early detection and treatment. ANC is also necessary to screen high risk pregnancy and high risk labor signs. The important components of antenatal care are discussed below:
Early Registration

The first visit of registration of a pregnant woman for Antenatal clinic (ANC) should take place as soon as the pregnancy is suspected; however very reporting in rural area was observed during the BLS survey. The Sticker drive for early registration was initiated in 30 villages in the project area.
Through this before sticking the stickers on the door of the beneficiaries; every married woman in the reproductive age group are encouraged to visit her nearest Sub Centre \ PHC or Private health provider or inform if he believes herself to be pregnant. Some pregnant woman who comes by themselves to the antenatal clinics that are organized on fixed days (arogya sessions) in intervention areas are registered and care is provided.
Ideally the first visit should take place in the first trimester (first three months of pregnancy), before or at the 12th week of pregnancy. However, if a woman comes late in her pregnancy for registration, she is encouraged and registered, and counselling is provided accordingly to her keeping her gestational age (duration pregnancy) and referred to PHC for further care. However many may not come. Regular field visits are paid to ensure all the pregnant women are registered and turn up for ANC check-ups in nearest aarogya sessions.
Early registration and ANC check-up of pregnant women is conducted with the help of medical officer and specialist gynecologist visits to
- Help the woman recall the date of her last menstrual period
- Assesses the health of the mother and to obtain baseline information on blood pressure (BP), weight and other vital signs.
- Screen for High risk pregnancy complications and manage them appropriately by referral and where required.
- Advice the woman to take first dose of tetanus toxoid injection (TT),well within time.(after 12 weeks of pregnancy)
- Administration of 2 doses of TT inj is given greater emphasis during the health check-ups. TT to a pregnant woman is an important step on the prevention of neonatal tetanus (tetanus of the newborn). The first dose of TT should be given just after the first trimester, or as soon as the woman registers for ANC whichever is later.TT injection is not to be given in the first trimester of pregnancy. the second dose is to be given one month after the first dose, but at least one month before the EDD.
- Help the woman access facilities for an early and safe abortion if she does not want to continue with her pregnancy
- Build a rapport between the pregnant woman and the project staff and heath workers.
The project coordinator and field supervisors with the help of various community based functionaries such as Anganwadi worker (AWW), the Traditional Birth Attendant (TBA)/Dai, members of Mahila Mandals, self-help groups, the panchayat and the village health committees who are likely to be aware of pregnant woman in the village are contacted and encourage them to update the list and help in providing ANC services.
Iron-Folic Acid(IFA) And Nutritional Supplementation :
During the arogya health sessions stress is given on the need for increased requirements of iron during pregnancy and inform the pregnant woman about the dangers of anemia during pregnancy.

- All pregnant women are encouraged to consume one tablet of IFA (100mg of elemental iron and 0.5mg of folic acid) every day for at least 100 days, starting after the first trimester at 14-16 weeks of gestation. This is the dose of IFA given to prevent anemia (prophylactic dose).
- If a woman is anemic (Hb<10g/dl) or she has pallor, she encouraged to consume two IFA tablets per day for 3 months. This means a woman with anemia in pregnancy needs to take at least 200 tablets of IFA during whole of pregnancy period. This is the dose of IFA required to correct anemia (therapeutic dose).
- Women with severe anemia (Hb<7g/dl) or those who have breathlessness and tachycardia (increased heart rate)due to anemia, are advice and started on the therapeutic dose of IFA and also referred to the doctor for further management.
Nutritional Advice In Pregnancy

Nutritional advice is given during the ANC clinic by Dr. Satalkar, Medical Officer. During which expected mother are explained about the nutritional requirements during pregnancy and for successful lactation. Following are some of the highlights
- The pregnant woman’s diet should provide for the needs of the growing foetus maintenance of the mother’s health, physical strength required during labour and successful lactation.
- Protein foods are essential for the growth of the foetus. If possible, the pregnant woman should take plenty of milk, eggs, fish poultry and meat. If she is vegetarian, she will need to have different cereals, a lot of pulses and nuts.
- Iron is very important for making the baby’s blood and to avoid or reduce incidence of anemia. She should have jaggery instead of sugar; eat ragi or bajra preparations, sesame seeds and plenty of dark green leafy vegetables. Liver and kidney are also rich in iron.
- Calcium is necessary for making the baby’s bones and teeth. The best source of calcium is milk. Calcium is also present in ragi and bajra; she should be encouraged to eat small dried fish.
- Vitamins are important for pregnant women. She should have plenty of vegetables (especially dark green leafy vegetables) and fruits including citrus kinds.
- Modified diets: In the presence of pregnancy induced hypertension or preeclampsia low salt diet is advised to prevent or reduce oedema. The woman may have a normal diet but avoid salted foods, and use little or no salt in cooking.
- High protein diet for preeclampsia, especially if there is albumin in the urine. The mother should be advised to increase her intake of protein foods.
Identification Of Transportation Facilities :
Recognised the fact that delays in reaching a healthcare facility is one of the major delays responsible for maternal mortality Lokmanya has introduced Emergency Medical Services in the project area.
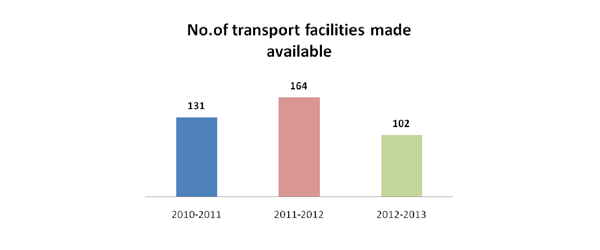
All the woman who has decided to deliver at a health facility, a vehicle is made available whenever the woman needs it, to take her to the health facility or referral centre; in case she develops some complications that need immediate referral and care.
All the Panchayat Village Health Committee, Mahila Mandals, SHG groups and Youth groups are informed about the services and explained them on how to obtain a vehicle in case of an emergency, if a vehicle is not available in the village. They were also informed about the JSSK schemes which are presently available for assisting the woman with transportation facilities.
Postpartum Clinic Visit
New mothers in the project area are identified by the field staff with the help of Anganwadi workers and encourage them to visit a health facility for her first postpartum visit, or be visited by a doctor at home, within 7 -10 days of delivery. This is especially true if she delivered at home.
All the ANC women are informed about the PNC first visit during field visits by Field Supervisors; as this is important to make sure that the woman and the infant are recovering from the labour and delivery. If all is well, the next visit should be about six weeks after the birth of the baby.
This was initiated with an objective that both the mother and infant have thorough physical examination and the infant is immunized. In addition this shall provide her an excellent opportunity to answer any questions the woman may have about breastfeeding, sexual relations, family planning, and immunization for the baby or other topics like Hygiene: Advise and explain to the woman not to insert anything into the vagina and to wash the perineum daily and after passing faeces. Perineal pads should be changed more frequently if there is heavy bleeding or for every 4 -6 hours. If cloth pads are used, the pads should be washed with plenty of soap and water and dried in the sun. She is also advised to take bath regularly and to wash her hands before handling the baby.
Family Welfare Programme (FWP):
Eligible couples, target couples and increasing couple protection rate:Family welfare programme (FWP) has been integrated with other health services instead of being a separate service. Family Welfare Programme can be successful only when it reaches those who are eligible and also those who are the targets. An eligible Target couple is a currently married cou¬ple, the wife being in the reproductive age group i.e. 15 to 45 year or who have had 2 to 3 living children. The definition of target couple has been gradually enlarged to include families with one child or even newly married couple. The aim is to develop acceptance of the idea of family planning from the earliest possible stage. Presently, it is estimated that there are 15000 eligible couples in the project area. Family planning was largely directed to such couples as these couples are in need of family planning services.
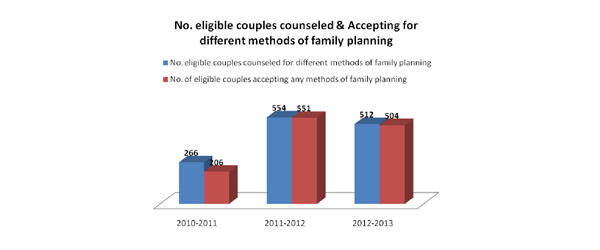
Eligible couples are approached by Field supervisors and project staff by house to house visit in the project area. Priority is given to motivation which is done at fixed day clinics and in hospital. Public are moti¬vated for post delivery sterilization and use of contracep¬tives. They are given contraceptives free of cost. Also sterilizations are done free of cost. Awareness on Child marriage re¬straint bill (1978), the age of marriage has been raised to 21 years for males and 18 years for females is undertaken during field visits and talks are arranged for adolescent girls,
Adolescent Girls Anaemia Control Program

Lokmanya initiated the “Adolescent Girls’ Anemia Control Program” for the adolescent girls in all the secondary and higher secondary sections of SNGO Project Area from November 2010.
Program Aims
- To institute school/Jr. College based, supervised weekly IFA supplementation with an in-built compliance monitoring system.
- To provide nutrition education to the beneficiary girls and teachers in order to effectively modify dietary behavior and thereby improve the intake of iron available from the food
Program Objectives
- To ensure that 90% of adolescent (12-19 year) girls in schools/ colleges and 70% of out-of-school participate in weekly consumption of IFA tablets under supervision
- Anemia prevalence in adolescent girls reduced by 90% by the end of the project period (three years).
- Improved dietary practices are observed in at least 25% of the adolescent girls both in and out of school setting by project end.
The second phase of the program was initiated in other remaining schools & Colleges covering over 1600 adolescent and especially reaching out-of-school girls through schoolgirls using girl-to-girl approach. The out-of-school girls are registered and informed about the anemia control programme launched by Lokmanya and asks them to collect medicines from the parivartak in their villages.
- Anemia prevalence in adolescent girls reduced by 40.25%
Adolescent Health & Hygiene
Several positive and negative lifelong behaviors are established during adolescence including diet and exercise, sexual conduct, practices related to oral health, smoking, drinking, and the use if legal and illegal substances. The complex issues that adolescents deal with on a daily
basis can turn into health problems that persist throughout adulthood. Unfortunately the adolescents who are frequently the most disconnected from routine health care services - those who lack insurance and family support - are often those at greatest risk for multiple and chronic health problems. Therefore, greater emphasis was given for addressing the health conditions that require immediate attention while preparing young people to adopt practices that can help improve their future health status and prevent unhealthy behaviors.
-
Adolescent Health BCC Training
- Lectures on Adolescents Health were organized with the help of Field Supervisors, Project Coordinator, anganwadi workers, School and Colleges. Dr. C.M. Gojamgunde, Public Health Specialist, Dr. Hemant Satalkar, Project Medical Officers delivered the lecture and answered the question raised by adolescent girls.
- Oath was delivered for – legal age of marriage/age of Ist conceiving
- Booklet on adolescent health was distributed to the college students
- Special Anemia intervention for girls below 12 mg (1 month intervention medicines, nutritional counseling, demonstration and supplementary food)/below 10 mg (3 month intervention medicines, nutritional counseling, demonstration and supplementary food) is initiated in five colleges.
-
Care of Out of School Adolescents Girls
- Adolescent period is a difficult emotional stage for boys and girls. Field Supervisors take group meetings separately for boys and girls where they are given health education and motivate out of school girls for screening for anemia.
- Filling up of prescribed format with 3 consecutive month’s recall of menstrual cycle.
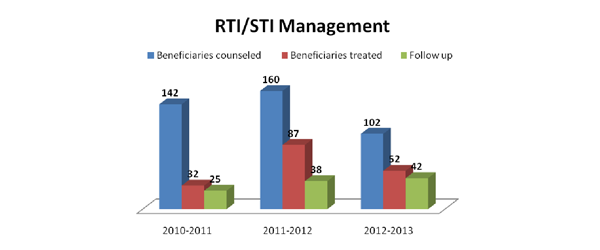
Lokmanya has organized on Site RTI/STI Clinic for provision of quality services for Syndromic management of STI & STD. Counselling and STI Clinic are regularly arranged by our project staff. Our Outreach workers and parivartaks create awareness on STI symptoms, identify the cases and encourage patients to seek treatment from our onsite STI/STD Clinic organized at mobile clinic.
Area Specific Activity School Health Appraisal Programme (Shape)

The school health service is defined as "the school procedures that contribute to the maintenance and improve¬ment of the health of pupils and school personnel including health services healthful living and health education".Lokmanya believes that; health education should be integrated with all the activities in
the -curriculum. It should be a part and parcel of the child's daily life. It must include the whole life of the child taking in to considera¬tion his relationship with the school community as well as the community outside the school.
School Health Annual Report Programme (SHARP), was started in July, 2010 with participation from government schools of project area of Khed Block. The programme was initiated with an objective to improve the acquisition of health related knowledge, attitudes, skills and practices and empower children.
Objectives of School Health Education:
-
The objectives of the school health education are as follows
- The promotion of positive health
- The prevention of diseases
- Early diagnosis, treatment and follow up of defects
- Awakening health consciousness in children
School health appraisal pro¬gramme comprising the following activities

- Health appraisal of school children and school personnel;
- Healthful school environment;
- Prevention of communicable diseases;
- Nutritional services;
- First aid and emergency care;
- Use of school health records;
- Remedial measures and follow up;
- Health instruction;
Health Appraisal:
The health appraisal covers not only the stu¬dents but also the teachers and other school personnel. Health appraisal consists of periodic medical examinations and observation of children by the class teacher.
The outcome of the SHAPE result have been satis¬factory for the following reasons

- A thorough medical examination of all pupils and necessary follow-up and treatment where necessary, is being carried out in all schools;
- Pupils with serious defects and those who suffer from severe illness are being examined more frequently; Medical examination is also given to teachers and other school personnel as they form a part of the school environment to which the children are exposed.
- The Teachers are advised to carry out the systematic 'daily inspection' and trained them in that; as teachers are in a unique position to carry out the 'daily inspection' as he is familiar with the children and can detect changes in the child appearance or behaviour that suggest illness or improper growth or development;
- This inspection must be made especially on the child's entry in the school premises in the morning and any change from the normal should be noted and correction may be made; in the same manner matters pertaining to cleanliness and neatness may also be noticed.
- School Health Activities Undertaken In Month Of December 2010 And January 2012
| Sr. No | Particulars | Conducted at | No. of Participants Attended |
|---|---|---|---|
| 1 | Sensitization of School Authorities on School Health and “systematic daily inspection' | Zilla Parishad School – Walad | 3 |
| Madhamik Vidyalaya | 2 | ||
| Zilla Parishad School – Kharoshi | 5 | ||
| Bhimashankar vidyalaya | 4 | ||
| New English School - Kohinde | 2 | ||
| Mamashaheb Mohol Madhamik Vidyalaya – Washere | 2 | ||
| Madhamik Vidyalaya – Saigaon | 3 | ||
| Govt. Ashram School – Chikhalgaon | 2 | ||
| Zp School – Mandoshi | 2 | ||
| Zilla Parishad School – Supewadi | 2 | ||
| Total No of Teachers Trained | 27 | ||
| Total no of School covered | 10 | ||
| 2 | School Health Check-up | ||
| School Health Check-up | Zilla Parishad School – Supewadi | 44 | |
Shape Outcome :
- Children pursue a healthy life, now and in the future.
- Work as agents of change for the improved health for their families and communities.
- Gain self reliance; develop positive self esteem and self assertiveness which enable them to cope with the pressures of a socio-culturally diverse and highly competitive world.
- Families also benefit by the vast pool of health information and skills that the child brings home from school, which can be used to improve knowledge, practices and conditions at home.
- Communities gain by acquiring increased awareness of health problems and their solutions through their involvement in school activities and community health projects.
It is seen that most of the students in the schools suffer from many preventable diseases such as defective teeth, bad sight, deafness, anaemia etc. but such diseases adversely affect the learning capacity of the students and cause ill health.
To conclude these data indicate that the commendable progress has been made in various key indicators in the project intervention area. However sustained efforts are required to ensure 100% full ANC coverage, Full Immunization and institutional deliveries in the inaccessible remote villages.